Squamous cell cancer is the second most common skin cancer. These cancers can grow rapidly & have the potential to spread to other areas. They are more frequent in elderly patients. The extreme UV index in Queensland predisposes patients to develop skin cancers, including SCCs. Early detection & treatment reduces mortality.
Key Points
- Squamous cell cancers are more dangerous than basal cell cancers
- These cancers mostly arise in sun exposed sites of the face & neck
- SCCs can potentially spread throughout the body if not treated
- Surgical treatments are indicated
- Photodynamic therapy can be used for non-invasive squamous cell cancers
- Your dermatologist will guide you as the most appropriate treatments
Squamous Cell Cancer Treatments at a glance
Best outcomes: 1-2 sessions
Procedure time: 15 -60 minutes
Duration of results: Remission
Back to work: Variable
Recovery: Variable
Anaesthetic: Local anesthetic
Your specialist: Dermatologist
How much: $ Medicare
Our results speak for themselves

Before
After

Obagi has medical grade therapy for acne. Benzoyl peroxide combined with active wash, cleanser & moisturizer
Ask us more about this treatmant
Preferred Consultation

Before
After

Medical therapy for acne
Ask us more about this treatmant
Preferred Consultation
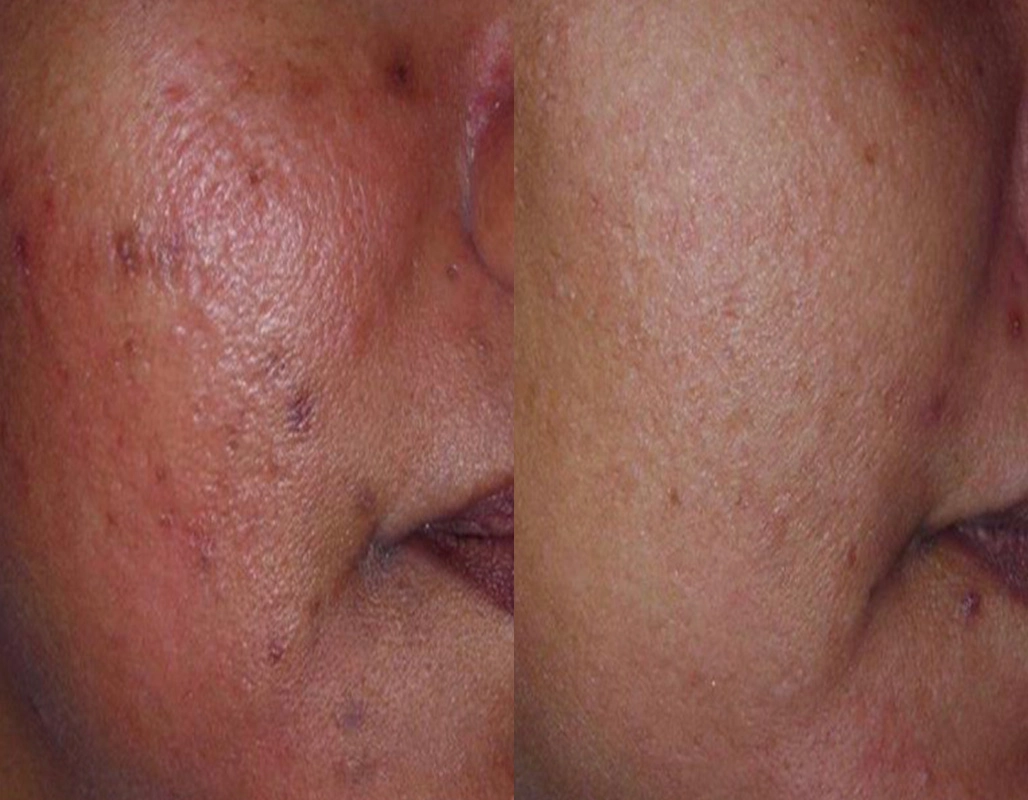
Before
After

Post inflammatory hyperpigmentation can be treated with lasers, topicals or chemical peels
Ask us more about this treatmant
Preferred Consultation
FAQs
What are squamous cell cancers?
SCCs or squamous cell cancers are the second commonest form of skin cancer, behind basal cell cancers. These cancers can rapidly grow in size & spread to distant sites if not diagnosed & managed early.
SCCs are mostly seen in elderly patients, however, can be seen at any age. These cancers appear exposed skin, especially scalps, ears, neck, & the backs of hands. They are also seen on the lips, particularly in smokers.
What do squamous cell cancers look like?
SCCs appear as a warty thickened lump often ulcerating or bleeding. They range in size from a few millimetres to centimetres. They commonly arise within pre-existing sun damaged skin. Solar keratosis or sunspots can be a precursor to squamous cell cancers.
How do dermatologists classify squamous cell carcinomas?
These cancers can be classified according to their level of ‘abnormal cells.’
- Well differentiated SCC tend to grow slowly with a very low chance of spread.
- Moderately differentiated SCC a slightly higher rate of growth and chance of spread than well differentiated tumours.
- Poorly differentiated SCC often rapidly growing and highly likely to spread if left untreated.
SCC are also more common in those with immune deficiencies, including transplant patients.
What do squamous cell cancers look like?
Squamous carcinomas tend to look like lumps arising from the skin with a scaly surface. They tend to grow over time. A rapidly growing SCC is often a variant known as a keratoacanthoma.
SCCs are commonly found on areas of the body which are more frequently exposed to sunlight, including the face, head, neck, & hands. Lower limb involvement is not uncommon.
How to treat squamous cell cancers?
Squamous carcinomas are most often treated with surgical excision.
The earlier your squamous cell carcinoma is diagnosed & treated, the less the cosmetic disfigurement & the less chance of recurrence or metastatic spread.
Are non-surgical treatments available for treating SCCs?
Non-surgical treatments including photodynamic therapy & Aldara are appropriate for thin, non-invasive SCCs known as intraepithelial carcinoma or SCC in situ. These treatments are not advocated for invasive squamous cell cancers.
In some cases, your dermatologist may opt for superficial radiotherapy to treat multiple cancers, or as adjuvant therapy for aggressive SCCs that involve high risk areas. Examples include SCCs with nerve spread or poorly differentiated squamous cell cancers.
What are keratoacanthomas?
KAs or keratoacanthomas are a variant of squamous cell cancers. These cancers grow rapidly, often doubling in size every 2-3 weeks. These cancers are mostly seen in elderly patients, on sun exposed sites. Unlike traditional SCCs, keratoacanthomas rarely spread, & frequently involute over 12 to 16 weeks. Treatment options include-
- Excision
- Curettage & cautery
- Superficial radiotherapy
- Intralesional chemotherapy
- Vitamin A tablets
These cancers are best managed by dermatologists, especially for patients with recurrent cancers.
What are the implications of SCCs in immunocompromised patients?
Immunocompromised patients include solid organ transplant, BMT, & genetic disorders predisposes patients to skin cancers. These patients have an excess of SCCs over BCCs which leads to a SCC/BCC ratio (2:1) that is reversed from what is usually reported in the general population (1:4).
This group is deemed high risk & are seen by dermatologists for higher level screening & management.
Products

Medik8 Physical Sunscreen SPF50+
$69.00

Dermaceutic All Things Pigment 21 Day Kit
$154.00
Early detection of SCCs confers an excellent prognosis. Early management of precancerous lesions such as solar keratosis can markedly reduce the chances of developing skin cancer.
How do dermatologists manage patients with multiple squamous cell cancers?
Our training enables us to manage high risk skin cancer patients. For this group, check-ups are conducted at 3-4 month intervals. We also consider chemoprophylaxis in high risk groups, including-
-
- Neotigison or Acitretin
- Field therapies
- Niacinamide supplementation
- Joint management with plastics & radiation oncologist
- Consideration of a change in immune suppression if indicated
What are the implications of smoking, lip cancer & squamous cell cancers?
SCCs on the lips are not infrequent in Brisbane – Queensland. The two main predisposing factors include smoking & UV radiation.
SCC on the lips have a higher rate of metastatic spread to distant sites- up to 20%. Early diagnosis & treatment reduces mortality.
What is the relationship between sunspots & squamous cell cancers?
Sunspots or actinic keratosis, also known as solar keratosis, are premalignant lesions. Sunspots have the potential to give rise to squamous cell cancers. The incidence ranges from less than 1% to 5%, depending on the literature review.
On this basis we advocate treatments of multiple solar keratosis as this reduces the incidence of skin cancers, but most importantly clears up sun damage to allow for early detection of clinically significant & possibly sinister lesions.
Can you die from squamous cell cancer?
SCCs can be associated with a high mortality rate, especially if picked up late. This especially applies to poorly differentiated squamous cell cancers on the head & neck, especially in immunocompromised patients.
High risk patients are seen every 3 to 4 months. In some cases, your dermatologist may consider methods to reduce the incidence of ‘squamoproliferative lesions’ including-
- Neotigison (vitamin A)
- Field radiation to areas (superficial XRT)
- PDT to field changes (photodynamic therapy)
Your dermatologist will often work with plastics, ENT, radiation oncologist & the Head & Neck team to manage your cancers.
How are dermatologists different from skin cancer doctors?
Dermatologists have an additional 5 years of formal education & expertise in the management of skin cancers, including squamous cell cancers. We manage skin cancers that are far beyond the level of experience of skin cancer general practitioners.
Our tertiary hospital training enables us to manage high risk patients, including immunosuppression, as well as rare & aggressive tumours.
What type of sunscreen is recommended for skin cancer prevention?
It is recommended to use a high factor of sunscreen no matter your skin type. SPF 50+ is recommended. The correct amount of sunscreen is equal to half to one teaspoon every 4-6 hours to cover the face & neck.
Good brands include Sun Sense, Neutrogena, Cancer Council & La Roche Posay.
Can vitamins reduce the rate of skin cancers including SCCs?
The prevention of common skin cancers including SCCs is possible by taking an inexpensive, widely available vitamin B3 supplement called nicotinamide. The dose is 500 mg twice a day. This can reduce squamous-cell cancers by 23%. Nicotinamide also reduced the risk for developing actinic keratosis, a common precancer of the skin.
Dr. Surana a dermatologist at Cutis Dermatology, Brisbane helped in the research on this ground-breaking treatment.
Ask us more about this treatment
Latest news
Insta code goes here
Insta code goes here
Insta code goes here